Polyp, Colonic
Management
Determine whether endoscopic resection is safely possible by the Kudo pit pattern classification system.
It requires magnification during colonoscopy using chromoendoscopy and evaluation of the pit pattern of the polyps. Pits are openings for the crypts.
The Kudo classification classifies pit pattern as round / normal (Type I), asteroid (Type II), tubular or round pit smaller than normal pit (Type IIIS), tubular or round pit larger than normal pit (Type IIIL), gyrus/dendritic (IV), irregular arrangement (VI), and loss of decrease of pits with amorphous structure (VN).
Polyps with type I to IV pit pattern are endoscopically resectable, while those with type VI and VN are suggestive of invasion and neoplasia.
Kudo Classification
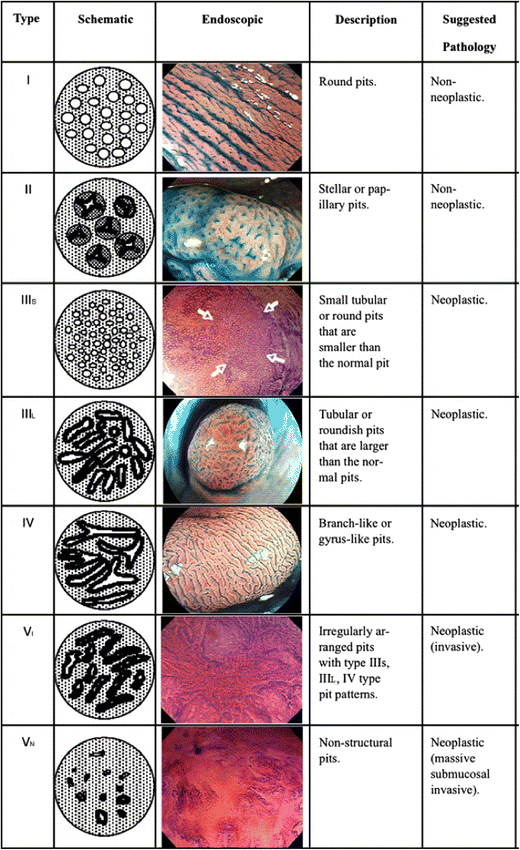
Resectable (TypeI-IV) <> Nonresectable (Type Vi &Vn)
+++++++++++++
Determine the optimal modality of endoscopic resection.
While studies have shown that there is only moderate agreement among experts when it comes to classifying large polyps according to various classifications,12 there are several available classifications.
In the US, the most commonly used are the Paris classification,13 narrow band imaging international colorectal endoscopic (NICE) classification,14 and Kudo’s classification of polyp pit pattern among others.15
Biopsy
++++++++++++++++++++
Adenomas should be resected completely.
Small adenomas (≤2 mm) may be completely removed using biopsy forceps,
Larger adenomas require snare resection, with or without electrocautery or
Cold snaring has the advantage of avoiding full thickness injury to the bowel wall that can accompany diathermy, and minimizes delayed postpolypectomy bleeding.
Large sessile adenomas often require piecemeal resection.
In cases where endoscopic resection is not possible, surgical resection is required. (See "Endoscopic removal of large colon polyps".)
Advanced endoscopic resection techniques (eg, endoscopic mucosal resection or endoscopic submucosal dissection) [84].
Pedunculated polyps with features of deep submucosal invasion should undergo endoscopic polypectomy with en bloc resection [79].
Nonpedunculated lesions with features of deep submucosal invasion should be biopsied in the area of surface feature disruption, tattooed if the polyps are not at or near the cecum, and patients should be referred for surgical management [79].
Nonpedunculated polyps with features of superficial submucosal invasion (eg, NG-LST morphology) should ideally be resected en bloc instead of piecemeal. In G-LST with a dominant nodule, the dominant nodule should be resected en bloc.
(See 'Endoscopic features and classification' above and "Endoscopic removal of large colon polyps", section on 'Features suggesting invasive cancer'.)